NP & PA Credentialing in Full, Reduced, and Restricted Practice States: What Providers and Healthcare Organizations Need to Know
NP & PA Credentialing in Full, Reduced, and Restricted Practice States: What Providers and Healthcare Organizations Need to Know | TriumpHealth
Credentialing nurse practitioners (NPs) and physician assistants/associates (PAs) is not a one-size-fits-all process. While every healthcare organization must verify education, licensure, board certification, malpractice coverage, work history, and clinical competence, the state practice environment plays a major role in how quickly and smoothly an NP or PA can be credentialed, privileged, and enrolled with payers.
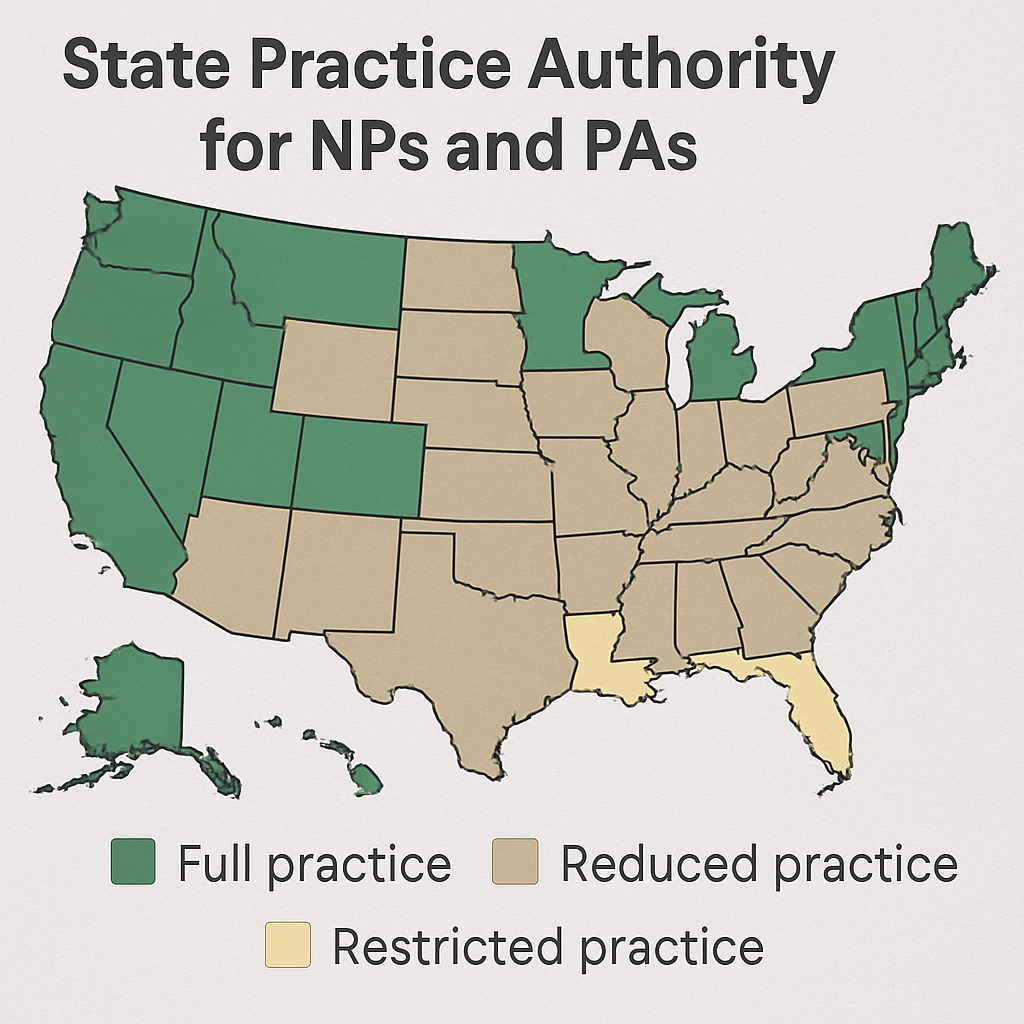
For mid-level providers, practice managers, and healthcare administrators, understanding the difference between full practice, reduced practice, and restricted practice states is essential. These classifications affect scope of practice, supervision or collaboration requirements, payer enrollment, billing workflows, privileging decisions, and compliance risk.
Whether your organization is hiring an NP, onboarding a PA, expanding into a new state, or opening a new service line, practice authority should be reviewed early in the credentialing process.
What Is Provider Credentialing?
Provider credentialing is the process of verifying that a healthcare professional is qualified to deliver care. For NPs and PAs, credentialing commonly includes verification of:
- Active state license
- Graduate education and professional training
- National certification
- Specialty qualifications
- DEA registration, when applicable
- State prescriptive authority
- Malpractice insurance
- Work history
- Clinical references
- Hospital affiliations or prior privileges
- Background checks and exclusions monitoring
- Continuing education and renewal status
For NPs and PAs, credentialing also requires a clear understanding of what the provider is legally allowed to do in the state where care is delivered. This is where full, reduced, and restricted practice environments become especially important.
Full Practice States: Credentialing Impact for NPs and PAs
In a full practice state, nurse practitioners generally have the authority to evaluate patients, diagnose conditions, order and interpret diagnostic tests, and initiate and manage treatment, including prescribing, under the authority of the state board of nursing. This model typically gives NPs the most independent practice authority.
For credentialing purposes, full practice authority usually creates a more streamlined process. The credentialing file focuses primarily on the NP’s own qualifications, licensure, certification, prescriptive authority, DEA registration, and competency. In most cases, there is no need to verify a physician supervision agreement or career-long collaborative arrangement.
For practice managers and administrators, this can reduce credentialing delays and simplify payer enrollment. NPs in full practice states may be easier to enroll as independent rendering or billing providers, depending on payer rules and organizational structure.
For PAs, the terminology is somewhat different. PA practice authority is typically tied to state laws governing collaboration, supervision, delegated authority, or practice-level decision-making. Some states allow more flexible PA team-based practice models, while others require more formal physician involvement. Even in states with modernized PA laws, organizations still need to verify the PA’s legal scope, collaboration requirements, prescriptive authority, and any physician relationship required by state law or payer policy.
Credentialing considerations in full or more autonomous practice environments
In full or more autonomous practice environments, credentialing teams should verify:
- NP or PA license status
- National certification
- Specialty training and experience
- State prescriptive authority
- DEA registration, if prescribing controlled substances
- Facility-specific privileging criteria
- Payer enrollment requirements
- Malpractice coverage
- Scope of services requested
- Quality and compliance standards
The key advantage is that the provider’s privileges are less likely to be tied to a specific supervising or collaborating physician. This can improve operational flexibility, especially for multi-site groups, telehealth organizations, urgent care centers, primary care practices, and specialty clinics.
Reduced Practice States: Credentialing Impact for NPs and PAs
In a reduced practice state, state law limits at least one element of NP practice or requires a regulated collaborative agreement with another healthcare provider. This does not necessarily prevent an NP from being credentialed or enrolled, but it does add documentation requirements.
For NPs, reduced practice states often require proof of a collaborative agreement, written practice agreement, protocol, or other state-required relationship. Credentialing teams must confirm that the agreement is current, compliant, signed by the appropriate parties, and aligned with the NP’s requested scope of practice.
For PAs, reduced or moderate practice environments may involve collaboration or supervision requirements, chart review standards, physician availability rules, prescribing limitations, or practice-level agreements. These requirements vary by state and may also vary by specialty or facility.
Credentialing considerations in reduced practice states
In reduced practice environments, organizations may need to collect and verify:
- Collaborative practice agreements
- Supervising or collaborating physician information
- Written protocols or delegation documents
- Prescriptive authority limitations
- Chart review or co-signature requirements
- Site-specific practice agreements
- Payer-specific collaboration documentation
- State board filing requirements, if applicable
The biggest credentialing challenge in reduced practice states is timing. An otherwise complete provider file may be delayed if the collaborative agreement is missing, expired, incomplete, or inconsistent with state law. Payer enrollment may also be delayed if the payer requires documentation of the collaborating physician relationship before approving the NP or PA as a rendering provider.
For administrators, reduced practice states require close coordination between credentialing, legal, operations, payer enrollment, and clinical leadership.
Restricted Practice States: Credentialing Impact for NPs and PAs
In a restricted practice state, NP practice is more dependent on physician supervision, delegation, or team management. These requirements may apply throughout the NP’s career and can significantly affect credentialing, privileging, and payer enrollment.
For NPs, restricted practice states often require more detailed documentation of the physician relationship. This may include supervision agreements, delegation protocols, chart review standards, prescribing delegation, or documentation showing that the NP is practicing within the limits established by state law.
For PAs, states with more restrictive supervision models may require a supervising physician relationship, limits on the number of PAs per physician, defined proximity requirements, chart co-signature rules, or board-approved delegation agreements. These requirements can directly affect whether the PA can begin seeing patients, prescribe medications, or practice at a specific site.
Credentialing considerations in restricted practice states
In restricted practice environments, credentialing files may need to include:
- Supervising physician agreement
- Delegation agreement
- Written protocols
- Proof of physician availability
- Chart review or co-signature process
- Prescribing delegation documentation
- Facility-specific supervision requirements
- Payer-specific supervision forms
- State board approvals or filings
- Updated agreements when physicians, locations, or service lines change
Restricted practice states typically create the highest administrative burden. Credentialing and privileging may be narrower, more dependent on a specific physician relationship, and more vulnerable to disruption if the supervising physician leaves the organization or changes roles.
For practice managers, this means credentialing should not be treated as a one-time onboarding task. Restricted practice environments require ongoing monitoring to ensure supervision agreements, delegation documents, and payer records remain current.
How Practice Authority Affects Payer Enrollment
Payer enrollment is closely connected to credentialing. Even after an NP or PA is licensed and internally credentialed, payers may require additional documentation before the provider can bill for services.
In full practice states, payer enrollment may be more straightforward because the provider’s authority is based more directly on licensure and certification. In reduced or restricted states, payers may request evidence of collaboration, supervision, delegation, or group affiliation.
Common payer enrollment issues include:
- Delayed enrollment due to missing supervision documents
- Incorrect provider taxonomy or specialty selection
- Confusion over billing versus rendering provider status
- Incomplete prescriptive authority documentation
- Mismatch between state scope of practice and requested services
- Expired collaborative or delegation agreements
- Failure to update payer records when a supervising physician changes
Administrators should review state practice requirements before submitting payer applications. Doing so can prevent avoidable denials, enrollment delays, and billing interruptions.
How Practice Authority Affects Hospital Privileging
Hospital and facility privileging determines what services an NP or PA may perform within a specific organization. Even when state law allows a provider to perform certain services, the facility must still approve privileges based on education, training, competence, experience, and organizational policy.
In full practice states, NP privileges may be granted based primarily on licensure, certification, training, and competency. In reduced or restricted states, privileges may also depend on the required physician relationship.
For PAs, privileging often reflects both the PA’s qualifications and the organization’s physician-led team structure. Facilities may require defined scope-of-practice documents, supervising physician acknowledgment, or service-line approval.
Credentialing committees should ensure that privileges are:
- Consistent with state law
- Supported by provider training and experience
- Aligned with payer billing rules
- Reflected accurately in internal policies
- Updated when regulations or provider roles change
- Compliance Risks in Reduced and Restricted Practice States
Reduced and restricted practice states create additional compliance risk because the provider’s authority may depend on documentation that must remain active and accurate.
Common compliance risks include:
- Lapsed collaborative agreements
- Outdated supervising physician information
- Missing delegation documentation
- Prescribing outside authorized scope
- Practicing at a location not covered by the agreement
- Failure to update payer records
- Inconsistent chart review or co-signature practices
- Privileges that exceed state-authorized scope
For NPs, PAs, and healthcare organizations, the most important compliance principle is alignment. The provider’s license, scope of practice, privileges, payer enrollment, employment role, and actual daily responsibilities should all match.
Best Practices for NP and PA Credentialing by Practice Environment
To credential NPs and PAs efficiently, healthcare organizations should build state practice authority into the credentialing workflow.
- Review state scope-of-practice rules before onboarding
Before extending privileges or submitting payer applications, confirm whether the state allows full, reduced, or restricted practice for NPs and what supervision or collaboration model applies to PAs.
- Collect supervision or collaboration documents early
In reduced and restricted states, do not wait until the end of credentialing to request collaborative agreements, delegation forms, or supervising physician documentation.
- Align payer enrollment with state law
Payer applications should accurately reflect whether the provider will bill independently, render services under a group, or practice under a supervising or collaborating physician arrangement.
- Keep agreements updated
When a supervising or collaborating physician changes, credentialing and payer enrollment files may need to be updated. This is especially important in restricted practice states.
- Match privileges to actual scope of practice
Hospital and facility privileges should reflect what the provider is trained, licensed, and legally permitted to do in that state.
- Monitor renewals and regulatory changes
State practice laws change over time. Organizations should periodically review NP and PA practice authority requirements, especially before expanding into new states.
Key Takeaways for Providers and Administrators
Full practice states generally create a more streamlined credentialing process for NPs because the provider’s authority is tied directly to licensure and board-regulated scope of practice.
Reduced practice states add credentialing requirements because collaboration or scope limitations must be documented and monitored.
Restricted practice states create the highest administrative burden because the provider’s authority may depend on ongoing physician supervision, delegation, or team management.
For PAs, practice authority varies by state and may involve collaboration, supervision, delegation, chart review, or practice-level agreements. Credentialing teams should review PA-specific state laws rather than assuming NP rules apply.
For practice managers and administrators, the credentialing process should always connect four key areas: state scope of practice, facility privileging, payer enrollment, and ongoing compliance.
Conclusion
NP and PA credentialing is directly affected by the state practice environment. In full practice states, credentialing is often more efficient because providers can practice with greater independence under their professional license. In reduced practice states, credentialing requires additional documentation around collaboration or limited scope. In restricted practice states, credentialing becomes more complex because supervision, delegation, and physician relationships may determine what the provider can legally do.
For healthcare mid-level providers, practice managers, and administrators, understanding these differences is essential for faster onboarding, cleaner payer enrollment, compliant privileging, and reduced operational risk.
Before hiring or credentialing an NP or PA, organizations should review the state’s current practice authority rules, payer requirements, facility bylaws, and any required supervision or collaboration agreements. A proactive credentialing strategy helps prevent delays, protects revenue, and supports compliant patient care across every practice environment. Let TriumpHealth handle the complexities of provider credentialing while you focus on patient care. Schedule a free consultation, email us at sales@triumphealth.com, or call (888) 747-3836 x0 to speak with a credentialing specialist today.